Introduction to Head and Neck Anatomy
| Site: | Newgate University Minna - Elearning Platform |
| Course: | Anatomy of Head and Neck |
| Book: | Introduction to Head and Neck Anatomy |
| Printed by: | Guest user |
| Date: | Friday, 10 July 2026, 1:02 AM |
1. Introduction to Head and Neck
The head and neck region is one of the most complex and vital areas of the human body. It houses critical sensory organs, the brain, major blood vessels, and structures essential for respiration, digestion, and communication. The study of this region provides insight into:
- Skeletal structures
- Soft tissues, including muscles, nerves, and vessels
- Functional compartments for protection, movement, and communication.
The head is the superior part of the body that is attached to the trunk by the neck. It is the control and communications centre as well as the “loading dock” for the body. It houses the brain; therefore, it is the site of our consciousness: ideas, creativity, imagination, responses, decision making, and memory. It includes special sensory receivers (eyes, ears, mouth, and nose), broadcast devices for voice and expression, and portals for the intake of fuel (food), water, and oxygen and the exhaust of carbon dioxide.
The head consists of the brain and its protective coverings (cranial vault and meninges), the ears, and the face. The face includes openings and passageways, with lubricating glands and valves (seals) to close some of them, the masticatory (chewing) devices, and the orbits that house the visual apparatus. The face also provides our identity as individuals. Disease, malformation, or trauma of structures in the head form the bases of many specialties, including dentistry, maxillofacial surgery, neurology, neuroradiology, neurosurgery, ophthalmology, oral surgery, otology, rhinology, and psychiatry.
2. The Cranium
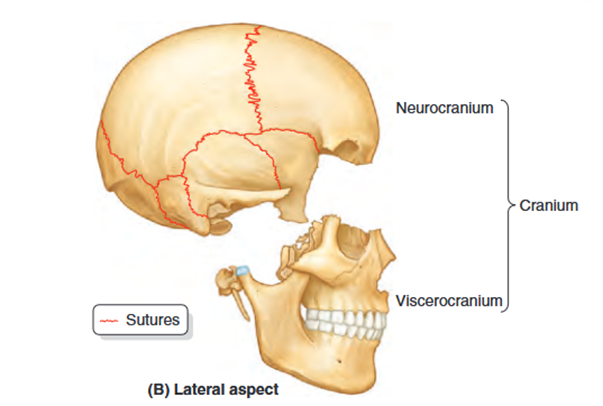
The cranium, or skull, serves as the skeleton of the head and is composed of two main parts: the neurocranium and the viscerocranium. The neurocranium encases the brain and its protective coverings, the cranial meninges, while also housing the proximal parts of cranial nerves and the brain's blood vessels. In adults, the neurocranium consists of eight bones: four singular bones aligned along the midline (frontal, ethmoidal, sphenoidal, and occipital) and two pairs of bilateral bones (temporal and parietal).
The neurocranium features a dome-like structure known as the calvaria, or skullcap, as well as a base referred to as the cranial base (basicranium). The calvaria is primarily made up of flat bones (frontal, parietal, and occipital) formed through intramembranous ossification of the head mesenchyme originating from the neural crest. In contrast, the bones that comprise the cranial base are mainly irregular bones with significant flat sections (sphenoidal and temporal), formed through endochondral ossification of cartilage (chondrocranium) or a combination of ossification types. The ethmoid bone, though irregular, contributes modestly to the midline structure.
Development of Cranium
The bones of the calvaria and some parts of the cranial base develop by intramembranous ossification. Most parts of the cranial base develop by endochondral ossification. At birth, the bones of the calvaria are smooth and unilaminar; no diploë is present. The frontal and parietal eminences are especially prominent. The cranium of a neonate is disproportionately large compared to other parts of the skeleton; however, the facial aspect is small compared to the calvaria, which forms approximately one eighth of the cranium. In the adult, the facial skeleton forms one third of the cranium. The large size of the calvaria in infants results from precocious growth and development of the brain and eyes. The rudimentary development of the face makes the orbits appear relatively large
Several bones of the cranium (frontal, temporal, sphenoid, and ethmoid bones) are pneumatized bones, which contain air spaces (air cells or large sinuses), presumably to decrease their weight. The total volume of the air spaces in these bones increases with age.
In the anatomical position, the cranium is oriented so that the inferior margin of the orbit and the superior margin of the external acoustic opening of the external acoustic meatus of both sides lie in the same horizontal plane. This standard craniometric reference is the orbitomeatal plane (Frankfort horizontal plane).
3. Areas of the Head
The head comprises several key areas, including the scalp, infratemporal fossa, pterygopalatine fossa, and cranial fossae. The scalp consists of skin (typically hair-bearing) and subcutaneous tissue that covers the neurocranium, extending from the superior nuchal lines on the occipital bone to the supra-orbital margins of the frontal bone. Laterally, it reaches over the temporal fascia to the zygomatic arches.
The scalp is organized into five layers, with the first three layers closely connected and functioning as a unit (e.g., when wrinkling the forehead or moving the scalp). The word "scalp" serves as a mnemonic for these layers:
- Skin: This thin layer, except in the occipital region, contains numerous sweat and sebaceous glands as well as hair follicles. It has a rich arterial supply and effective venous and lymphatic drainage.
- Connective Tissue: This thick, dense layer is richly vascularized and well-supplied with cutaneous nerves, forming the subcutaneous layer.
- Aponeurosis (epicranial aponeurosis): A broad, strong tendinous sheet covering the calvaria, it serves as the attachment point for muscle bellies from the forehead and occiput (occipitofrontalis muscle) and from the temporal bones (temporoparietalis and superior auricular muscles). Together, these make up the musculoaponeurotic epicranius. The frontal belly of the occipitofrontalis pulls the scalp forward, wrinkles the forehead, and elevates the eyebrows, while the occipital belly pulls the scalp backward, smoothing the forehead skin. The superior auricular muscle elevates the auricle of the external ear. All components of the epicranius are innervated by the facial nerve.
- Loose Areolar Tissue: This sponge-like layer contains potential spaces that can fill with fluid due to injury or infection. It allows for the free movement of the scalp proper (the first three layers) over the underlying calvaria.
- Pericranium: A dense connective tissue layer forming the external periosteum of the neurocranium. Although it is firmly attached, it can be easily stripped from the skull in living individuals, except where it is continuous with fibrous tissue in the cranial sutures.
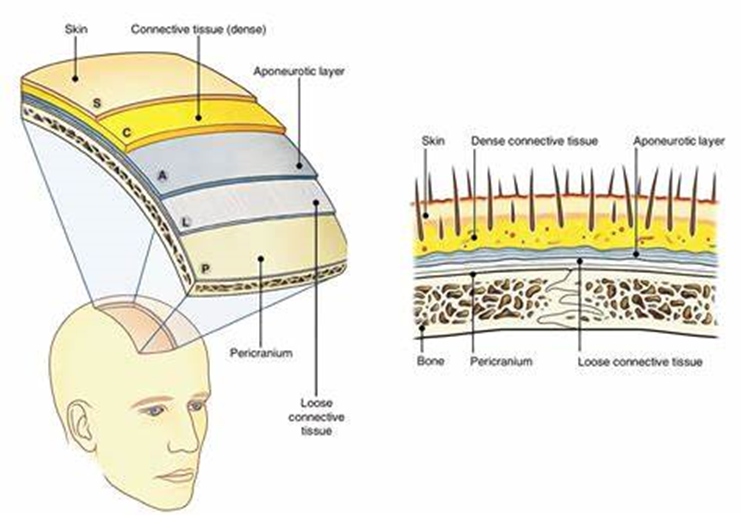
The three outermost layers move as one unit, with the aponeurosis being a tendon-like structure spanning between the frontalis and occipitalis muscles.
The scalp receives a rich arterial supply from the external carotid artery, and sensory innervation from the trigeminal nerve, as well as cervical nerves.
The infratemporal fossa is a complex area located at the base of the skull, deep to the masseter muscles. The infratemporal fossa provides a conduit for neurovascular structures entering and leaving the cranial cavity.
4. Surfaces of the Skull
Facial Surface: Features of the anterior or facial (frontal) aspect of the cranium are the frontal and zygomatic bones, orbits, nasal region, maxillae, and mandible.
The frontal bone, specifically its squamous (flat) part, forms the skeleton of the forehead, articulating inferiorly with the nasal and zygomatic bones. In some adults a frontal suture persists; this remnant is called a metopic suture. It is in the middle of the glabella, the smooth, slightly depressed area between the superciliary arches.
The frontal or metopic suture divides the frontal bones of the fetal cranium into two left and right.
The intersection of the frontal and nasal bones is the nasion, which in most people is related to a distinctly depressed area (bridge of nose). The nasion is one of many craniometric points that are used radiographically in medicine (or on dry crania in physical anthropology) to make cranial measurements, compare and describe the topography of the cranium, and document abnormal variations. The frontal bone also articulates with the lacrimal, ethmoid, and sphenoid; a horizontal portion of bone (orbital part) forms both the roof of the orbit and part of the floor of the anterior part of the cranial cavity.
The supra-orbital margin of the frontal bone, the angular boundary between the squamous and orbital parts, has a supra-orbital foramen (notch) in some crania for passage of the supra-orbital nerve and vessels. Just superior to the supra-orbital margin is a ridge, the superciliary arch, that extends laterally on each side from the glabella. The prominence of this ridge, deep to the eyebrows, is generally greater in males.
The zygomatic bones also known as “cheek bones, malar bones”, forming the prominences of the cheeks, lie on the inferolateral sides of the orbits and rest on the maxillae. The anterolateral rims, walls, floor, and much of the infra-orbital margins of the orbits are formed by these quadrilateral bones. A small zygomaticofacial foramen pierces the lateral aspect of each bone. The zygomatic bones articulate with the frontal, sphenoid, and temporal bones and the maxillae.
Inferior to the nasal bones is the pear-shaped piriform aperture, the anterior nasal opening in the cranium. The bony nasal septum can be observed through this aperture, dividing the nasal cavity into right and left parts. On the lateral wall of each nasal cavity are curved bony plates, the nasal conchae.
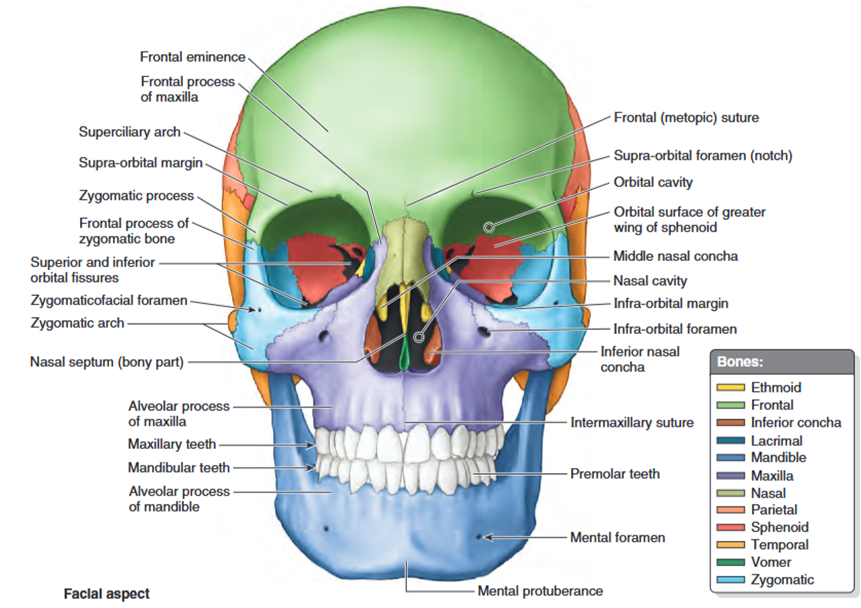
The maxillae form the upper jaw; their alveolar processes include the tooth sockets (alveoli) and constitute the supporting bone for the maxillary teeth. The two maxillae are united at the intermaxillary suture in the median plane. The maxillae surround most of the piriform aperture and form the infra-orbital margins medially. They have a broad connection with the zygomatic bones laterally and an infra-orbital foramen inferior to each orbit for passage of the infra-orbital nerve and vessels.
The mandible is a U-shaped bone with an alveolar process that supports the mandibular teeth. It consists of a horizontal part, the body, and a vertical part, the ramus. Inferior to the second premolar teeth are the mental foramina for the mental nerves and vessels
The mental protuberance, forming the prominence of the chin, is a triangular bony elevation inferior to the mandibular symphysis, the osseous union where the halves of the infantile mandible fuse.
- Key Bones: Maxilla, zygomatic, nasal, vomer, palatine, and mandible.
- Features: Includes the orbits (eye sockets), nasal aperture, and oral cavity.
- Function: Supports facial expressions, mastication, and housing of sensory organs (eyes, nose, mouth).
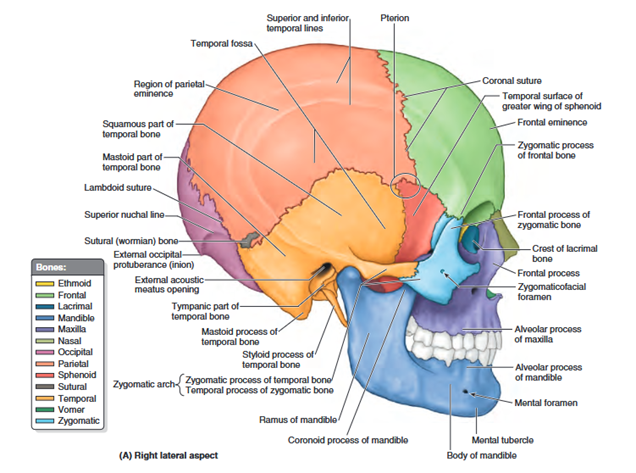
Lateral Surface
The lateral aspect of the cranium is formed by both neurocranium and viscerocranium.
The main features of the neurocranial part are the temporal fossa, the external acoustic meatus opening, and the mastoid process of the temporal bone. The main features of the viscerocranial part are the infratemporal fossa, zygomatic arch, and lateral aspects of the maxilla and mandible.
The temporal fossa is bounded superiorly and posteriorly by the superior and inferior temporal lines, anteriorly by the frontal and zygomatic bones, and inferiorly by the zygomatic arch. The superior border
- Key Bones: Temporal, parietal, frontal, and sphenoid.
- Landmarks:
Pterion: The junction of frontal, parietal, temporal, and sphenoid bones.
External acoustic meatus: Opening for the ear canal.
Zygomatic arch: Formed by the zygomatic and temporal bones.
- Clinical Note: The pterion is a vulnerable area; fractures can damage the middle meningeal artery, leading to epidural hematoma.
Occipital Surface: The posterior or occipital aspect of the cranium is composed of the occiput (back of head, the convex posterior protuberance of the squamous part of the occipital bone), parts of the parietal bones, and mastoid parts of the temporal bones.
The external occipital protuberance is usually easily palpable in the median plane; however, occasionally (especially in females) it may be inconspicuous. A craniometric point defined by the tip of the external protuberance is the inion. The external occipital crest descends from the protuberance toward the foramen magnum, the large opening in the basal part of the occipital bone.
- Key Bone: Occipital bone.
- Features:
External occipital protuberance: Palpable bony prominence.
Foramen magnum: Large opening for the spinal cord.
Occipital condyles: Articulates with the atlas (C1 vertebra).
- Function: Provides attachment for neck muscles and allows communication between the cranial and spinal cavities.
Superior External Surface
- Bones Involved: Frontal, parietal, and occipital.
- Landmarks:
Sagittal suture: Between parietal bones.
Coronal suture: Between frontal and parietal bones.
Lambdoid suture: Between parietal and occipital bones.
- Clinical anatomy: Sutures in adults are fused; in infants, they allow for skull expansion during growth.
2.5 Internal Surface of the Cranium
- Features:
Divided into three cranial fossae: anterior, middle, and posterior.
Anterior cranial fossa: Contains the frontal lobes; notable structures include the crista galli and cribriform plate.
Middle cranial fossa: Houses the temporal lobes; notable structures include the sella turcica and foramen ovale.
Posterior cranial fossa: Contains the cerebellum and brainstem; notable structures include the jugular foramen and hypoglossal canal.
Walls of the Cranial Cavity
- Structure:
Outer table: Dense, compact bone.
Diploë: Spongy bone with venous channels.
Inner table: Thin, brittle compact bone.
- Clinical anatomy: The thin inner table makes the cranial cavity susceptible to fractures and intracranial complications.
5. The Face
The face is the anterior part of the head, extending from the forehead to the chin and from one ear to the other. It serves as a key aspect of our identity, making alterations due to birth defects, scarring, or trauma have significant emotional and psychological consequences beyond their physical implications.
The fundamental shape of the face is determined by the underlying bones, while its individuality arises from anatomical variations in the shape and prominence of facial features, the deposition of fatty tissue, skin color, aging effects, and the nature and placement of hair on the face and scalp. In infants, the relatively large buccal fat pads help maintain cheek fullness during sucking, giving them a chubby appearance.
Facial bones grow more slowly than those of the calvaria. By the age of seven, the ethmoid bone, orbital cavities, and upper parts of the nasal cavities are nearly fully developed. As the orbits expand and the nasal septum grows, the maxillae move infero-anteriorly. Considerable facial growth continues throughout childhood, coinciding with the development of paranasal sinuses and the eruption of permanent teeth.
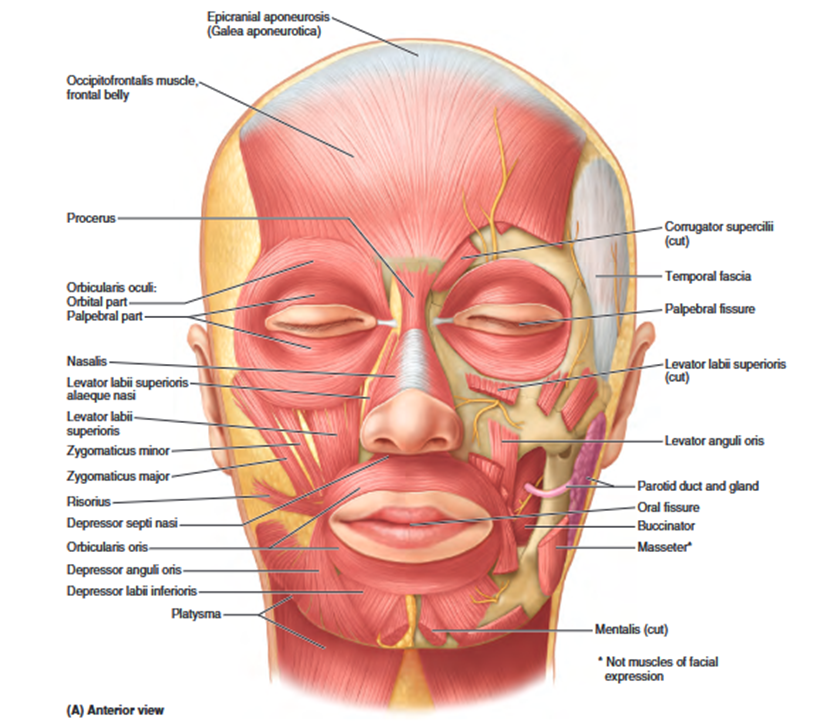
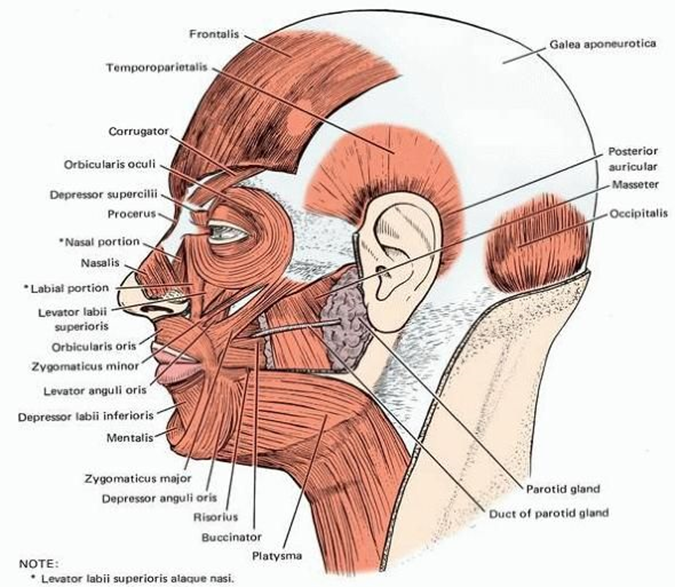
The face is essential for communication, serving as the primary interface for our interactions with others. While the shape and features of the face establish our identity, much of the impact we have on others and their perceptions of us come from how we utilize facial muscles to create subtle alterations in our expressions.6. Muscles of the Face and Scalp
The facial muscles, also known as the muscles of facial expression, are located in the subcutaneous tissue of the anterior and posterior scalp, face, and neck. These muscles enable movement of the skin, allowing for the alteration of facial expressions to communicate emotions. Most of these muscles attach to either bone or fascia and function by pulling the skin.
All facial expression muscles originate from the mesoderm in the second pharyngeal arches. During embryonic development, a subcutaneous muscular sheet forms that extends over the neck and face, incorporating branches of the facial nerve (CN VII) to innervate the muscles derived from the arch. This muscular sheet differentiates into muscles that encircle the facial openings such as the mouth, eyes, and nose hence acting as sphincters and dilators, while also facilitating a variety of facial expressions. Due to their shared embryological origin, the platysma and facial muscles often fuse, resulting in intermingled fibres.